
Diagnosing Canine Diabetes
Diabetes mellitus is not the only cause of polyuria/polydipsia and weight loss. Each dog should be examined thoroughly to rule out any other causes before starting insulin management. A preliminary diagnosis of diabetes mellitus, based on clinical signs, must be confirmed by blood and urine tests. Reference values for blood glucose range from 4.4 to 6.7 mmol/l in dogs. The renal threshold is around 11-12 mmol/l. If the blood glucose concentration exceeds this threshold, glucose is excreted in the urine.
Presentation of a non-complicated dog with diabetes
Types of patients categorised as non-complicated and therefore not emergencies:
- Dogs presented to the vet after the dog owner has noted the appearance of clinical signs without general deterioration—that is, no diabetic ketoacidosis (DKA).
- Dogs that, after initial presentation with DKA and its successful treatment, are generally stable and without ketonuria.
Healthy diabetes management
The goals in managing diabetes mellitus are to minimise the clinical signs of diabetes, the risk of hypoglycaemia, and the development of long-term complications.
Accomplishing these goals requires that dog owners understand all aspects of diabetes management. Investing enough time to conduct a careful explanation of all the aspects of the therapy is strongly recommended.
Managing diabetes can be, at times, challenging, until stabilisation occurs; however, there are tools available to help evaluate the disease and its management, and there are resources available through this website to provide additional support. Insulin therapy forms one of the cornerstones of the management of diabetes mellitus; therefore, it is important to understand the length of action of insulin and how to evaluate management.
Evaluation of management
Monitoring blood glucose is a good way to evaluate regulation of a dog with diabetes. It is accurate, rapid and requires only a drop of blood. However, in certain conditions (see below) it is not reliable because blood glucose concentration is influenced by many factors. Consequently, blood glucose curves may not show the actual effectiveness of insulin treatment and should always be interpreted in conjunction with clinical signs.
Various factors such as economics, logistics, and clinical situations can also force vets to limit diagnostic procedures. When it is not possible to perform a complete glucose curve, or use a device to monitor interstitial glucose, then a small series of blood samples taken in the middle of the day, combined with clinical signs, general observations and evaluating glycosuria can provide an overview of the animal's diabetic control.
Vets can also rely on evaluation of glycosylated proteins: glycosylated haemoglobin (GHb) and fructosamine, in laboratory testing.
Glycosylated proteins
Measurement of the glycosylated proteins serum fructosamine (SF) and glycosylated haemoglobin (GHb) is another way to evaluate diabetic stability. The level of these proteins reflects the chronic hyperglycaemia characteristic of diabetes mellitus and are not affected by stress, medication or recent feeding. SF is most frequently used and reflects the regulation of mean blood glucose levels for 1-3 weeks before the blood sample1.
Blood samples to assess SF levels in the dog can be taken at any time of day and only a single sample is required, however there are limitations and results should be interpreted accordingly:
- Serum fructosamine analysis is unable to detect short-term or transient abnormalities in the blood glucose concentration, e.g. transient daily episodes of hypoglycaemia. This would require serial measurement of blood glucose concentrations.
- Albumin and fructosamine concentrations are highly correlated in dogs. Dogs with hypoalbuminemia also have a decreased fructosamine concentration (false negative)—the laboratory performing the analysis should be consulted as to whether a correction is required and if this has been done.
Available management tools
- Glucose curves
- Serial blood samples
- Evaluation of glycosuria and monitoring
- Clinical signs
- Glycosylated hemoglobin and fructosamine
Certain conditions
Food intake, exercise, use of some medications (e.g. xylazine, medetomidine, prednisolone, progestogens) and other conditions (e.g. hyperadrenocorticism) or stress can affect blood glucose levels. In these cases, blood glucose measurement will not be helpful and other methods of evaluation should be used.
-
Clinical Signs
Signs presented by dogs with diabetes
Clinical signs exhibited by dogs with diabetes reflect the underlying pathological mechanisms of the disease and aid diagnosis. Laboratory tests are needed to confirm diagnosis.
Three distinct clinical pictures in diabetes mellitus
- Uncomplicated
- Complicated by ketoacidosis
- Hyperosmolar syndrome
Classical signs of uncomplicated diabetes mellitus- Polyuria/polydipsia
- Polyphagia
- Weight loss
- Increased susceptibility to infections (e.g. urinary tract infections)
Additional signs of diabetes mellitus complicated by ketoacidosis- Severe depression
- Anorexia
- Vomiting
- Dyspnoea
- Collapse or coma
Signs of hyperosmolar syndromeIn those dogs in which resistance of target tissues to insulin plays a key role in the disease, insulin levels can be elevated. In these cases, ketosis is suppressed, and plasma glucose concentrations can become very high. Dogs with hyperosmolar syndrome are usually comatose on presentation.
-
Differentiating Factors
Common factors associated with diabetes mellitus
Weight loss despite a good appetite
Noticeable weight loss in a dog may cause a concerned pet owner to visit their vet. Although diabetes is a common diagnosis in dogs that have lost a significant amount of weight, other factors that can cause this should be considered. The following algorithm can be used to help determine an accurate diagnosis2.

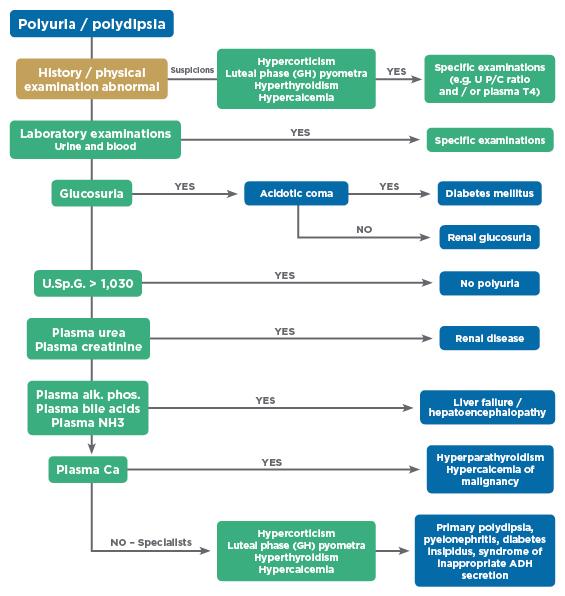
Polyuria/polydipsia
It is common for dog owners to seek veterinary support when their dog is urinating in the house and/or consuming large amounts of water. Although diabetes mellitus is a well-known cause of polyuria and polydipsia, there are many other factors to consider. The following algorithm can be used to help determine the cause of the problem2.

-
Managing Uncomplicated Diabetes
Appearance & Management of Uncomplicated Diabetes
Two types of patients can be categorised as uncomplicated:
- Dogs presented to their vet after the owner has noted the appearance of clinical signs and without general deterioration (no diabetic ketoacidosis (DKA). These cases are not emergencies, although dogs without complications should be treated diligently to try to reduce the possibility of them occurring in the future.
- Dogs that have had an initial presentation with DKA but have been treated successfully and are generally stable, without ketonuria.
During consultation:
- Perform a thorough examination, weigh the patient and record the Body Condition Score (BCS).
- Conduct laboratory testing, including a complete blood count, urinalysis (including sediment examination) and a serum biochemistry profile.
- If the clinical examination or initial biochemistry screening indicates there could be underlying conditions, rule out hypothyroidism, renal failure, inflammatory bowel disease, pancreatitis, exocrine pancreatic insufficiency, hyperadrenocorticism, neoplasia or hepatic disease as appropriate.
When the general health status is known, and diabetes mellitus is confirmed:
- It is important to explain that achieving stabilisation in patients with diabetes mellitus, may take time (up to 6 months) and what the implications are for the dog owner and family. Make sure the owner understands the therapy involved and that the dog should be able to live a happy, healthy life with consistent management. This is crucial, as complete cooperation of the owner is essential to successful management.
- Treat existing infections or other medical conditions as many concurrent diseases can affect insulin metabolism.
- Evaluate the current diet and consider changing it if appropriate.
- Begin therapy with Caninsulin® (porcine insulin zinc suspension).
-
Starting Caninsulin Therapy
Determine the owner-preferred method of administration
Caninsulin can be given via two methods of administration
Vetpen® is the first and only insulin pen to deliver 40 IU/ml insulin via 2.7ml cartridges. This method is more accurate than the traditional syringe approach and is easy to use3,4.
Caninsulin is also available in 2.5ml and 10ml vials for use with specific 40 IU syringes.
Steps in clinic
- Establish a starting dose by weighing the dog.
- Hospitalise for the day to verify that the starting dose does not cause hypoglycaemia.
- Instruct dog owner on:
- Injection technique.
- How to identify and treat hypoglycaemia if it occurs.
- Introduce the diabetes tracker app to help the pet owner record their dog’s diabetes information more effectively.
- The pet should then be sent home for 1 week to allow the owner, the family and dog to become accustomed to managing diabetes.
Make sure pet owners have a specific contact at the clinic, often a veterinary nurse, who is available for phone calls or further clinic visits should the client feel unsure.
Some owners may struggle with the idea of injecting their pet at home, without the support of clinic staff and they may prefer to bring their pet in on a daily basis for the first few days. The veterinary nurse can observe injection technique, VetPen handling and alleviate the reasons for concern. Positive reinforcement by a health care professional will increase client confidence and enable them to proceed at home.
Tasks for clients at home
- Monitor and record daily water and food consumption.
- Maintain starting dose and frequency of administration for the entire week.
- Watch for signs of hypoglycaemia.
- Consider monitoring and recording urine glucose and ketone concentrations at regular intervals – this may be an important consideration in cases where urinary ketones have been previously recognised.
Clinic re-evaluation after one week- Verify adequate injection technique.
- Evaluate dog owner's monitoring of clinical signs and glucosuria.
- Weigh and body condition score the patient.
- Evaluate glycaemia via glucose curve or serial blood glucose evaluations (3 to 4 samples taken around midday).
- Increase insulin dose if necessary, according to clinical signs and glycaemia values, if evaluated. Ensure an interval of no less than 3 days (ideally around 7-10 days) between dosage increments. Changing the dose more frequently than that can lead to Somogyi overswing.
Ongoing regulation- Repeat procedures listed above at regular intervals until clinical signs and body weight/body condition score are satisfactory and the owner reports that they and their dog are enjoying a good quality of life.
- When stabilisation is achieved (no clinical signs; satisfied owners), it is suggested to schedule rechecks every 2 to 4 months:
- Perform a complete physical examination, including weight and body condition score evaluation.
- Revise home monitoring if necessary.
- Evaluate glycaemia if necessary (e.g. glucose curve, serum fructosamine).
Problems
If clinical signs resume, the blood glucose curve and serum fructosamine levels are not satisfactory and/or there is deterioration of overall health, causes must be identified.
- Perform a complete physical examination.
- Recheck:
- Injection technique and insulin quality control.
- Feeding and exercise.
- Environment of the patient (especially any recent changes).
- Perform a glucose curve.
- Evaluate a complete blood count, urinalysis (including sediment examination) and serum biochemistry profile.
- Additional testing procedures may be required, such as a T4 analysis and ACTH stimulation or low dose dexamethasone test to eliminate concurrent diseases that may have an impact on the efficacy of insulin.
-
Managing Diabetes Complicated by Ketoacidosis
Diabetic ketoacidosis (DKA) is potentially life-threatening
Diabetic ketoacidosis (DKA) is a severe form of complicated diabetes mellitus which requires emergency care. Ketones are synthesised from fatty acids as a substitute form of energy, because glucose has not effectively entered cells. Excess ketoacids results in acidosis and severe electrolyte abnormalities, which can be life threatening. If a diagnosis of DKA is made, aggressive and immediate treatment is required.
Diagnosis
The diagnosis is based on clinical signs – those of severe, untreated diabetes mellitus (particularly severe dehydration) the presence of glucosuria, proteinuria and ketonuria alongside confirmatory biochemical blood analysis.
Management guidelines
Goals of treatment include the rapid correction of fluid deficits, acid-base balance and electrolyte balance, the reduction of blood glucose and ketonuria, the commencement of insulin therapy and the management of concurrent diseases.
Many protocols for treatment exist but rapid-acting insulin (regular) must be administered first to reduce the hyperglycaemia as quickly as possible, ensuring that the blood glucose concentrations do not decline below 12 mmol/l for the first 24-48 hours of therapy, as lower values may predispose the patient to development of cerebral oedema5,6. Once blood sugar levels have been lowered and maintained at 11-14 mmol/l for 4−10 hours, then Caninsulin® (porcine insulin zinc suspension) can be started.
Evaluation of treatment
When evaluating the regulation of insulin therapy following an episode of DKA, it is important to consider several areas including the evaluation of glycaemia (via a blood glucose curve where possible), urine monitoring, regular rechecks and, longer term, glycated protein evaluations.
Most dogs will return home after appropriate DKA management, including a few days in the hospital, and make a full recovery back to a stable diabetic. Some dogs will have recurrent DKA episodes and these patients should be checked thoroughly for underlying conditions.
Routine re-checks
After the animal has been stabilised successfully, routine rechecks should be performed at regular intervals (2−4 months) on regulated animals. Recheck evaluations will sometimes reveal slight hypo- or hyperglycaemia and if all other parameters (urine, appetite, water uptake, general conditions, etc.) are normal, repeat testing of the glucose the following day and closer evaluation of other parameters is recommended before any adjustment of the dose is made.
The use of glycosylated proteins following an episode of DKA
Glycosylated proteins, such as serum fructosamine (SF), can also be a useful diagnostic tool to use for a few months following an episode of DKA, but should not be used in place of good monitoring of clinical signs. The level of these proteins reflects the chronic hyperglycaemia characteristic of diabetes mellitus and is not affected by stress, medication or recent feeding. SF is most frequently used and reflects the mean blood glucose for 1-3 weeks before the blood sample was taken. A normalising of the SF level over the following month or two suggests the dog is now stable and less likely to suffer from further complications.
-
Managing Hyperosmolar Syndrome
Proper management to avoid complications
Diabetic hyperosmolar (nonketotic) syndrome (DHNS) is a complication of diabetes mellitus that is not commonly observed in the dog. It is a potentially serious development in dogs with diabetic ketoacidosis (DKA) and can have profound effects on the function of the central nervous system.
Diagnosis
Physical examination often reveals profound dehydration, and the dog is typically lethargic, extremely depressed, or comatose. There is a direct relationship between the severity of the hyperosmolality and the severity of these signs.
Affected dogs exhibit the classic signs of diabetes mellitus (polydipsia, polyuria, polyphagia, and weight loss). They progressively get weaker, experience anorexia, become lethargic and drink less fluids.
Management guidelines
Goals of management include the correction of any fluid deficits and electrolyte imbalance associated with severe dehydration, the reduction of blood glucose via insulin therapy, correction of the hyperosmolar state and management of concurrent diseases.
Hyperosmolality usually resolves with intravenous isotonic fluid and insulin therapy, although correction of the hyperosmolar state must be done slowly to minimise the shift of water from the extracellular to the intracellular compartment. Fluid therapy is critical to manage DHNS, especially in the first 4 to 6 hours of management.
The normal range of serum osmolality in a dog is typically 280 to 300 mOsm/kg.
The goal is to reduce blood glucose at the rate of 2.5 to 3 mmol/l/hr. When the blood glucose approaches 14.0 mmol/l, the IV fluid selection should be changed to 5% dextrose solution. Insulin therapy should be delayed (typically 4 to 6 hours) until the fluid therapy has improved the condition of the dog, corrected the dehydration, hyperglycaemia, hyperosmolality and electrolyte balance and improved urine production7. The need for insulin management is not as critical with hyperosmolar nonketotic syndrome as with ketoacidosis.
Evaluation of management
When evaluating fluid therapy, it is important to consider several areas including urine monitoring, blood pressure, blood glucose, serum electrolytes, blood urea nitrogen (BUN) and urine glucose.
-
Related Diseases
Diseases that may contribute to the development of diabetes
Dioestrus diabetes
In entire, cycling female dogs, the onset of dioestrus diabetes is believed to be induced by increases in circulating progesterone levels (and potentially also mammary gland-derived growth hormone concentrations) during the dioestrus phase of the normal hormone cycle. Both progesterone and growth hormone cause insulin resistance and may induce diabetes mellitus in the luteal phase of the cycle.
Serum fructosamine levels may well be normal as serum glucose levels are likely to have been in the normal range prior to the dioestrus phase and diagnosis is based on a history of rapid onset clinical signs alongside hyperglycaemia and glycosuria.
Once the dog is stable, it is important to perform an ovariohysterectomy and then monitor blood glucose levels carefully as some dogs may not require insulin long-term.
Exocrine pancreatic insufficiency (EPI)
Exocrine pancreatic insufficiency is a congenital or acquired condition that can affect both dogs and cats, although it is more common in dogs. Young adult dogs, especially German Shepherds, are usually affected. In dogs, EPI is usually due to pancreatic acinar atrophy (PAA). It may be seen together with diabetes mellitus if there is damage to both the exocrine and endocrine pancreas.
Pathophysiology
- Digestive enzymes are not secreted normally by the pancreas.
- Food is not sufficiently digested and processed.
- Diarrhoea and weight loss occur despite a normal or increased appetite.
Diagnosis and treatmentEPI is diagnosed based on blood tests and is treated with pancreatic enzyme replacements. Enzyme replacements usually result in improvement of the clinical signs, and dietary management. However, if due to chronic pancreatitis and accompanied by diabetes mellitus, it can be more difficult to treat successfully.
Hyperadrenocorticism (Cushing’s disease)
Hyperadrenocorticism is a relatively common endocrine disease of dogs.
Aetiology
- Excessive endogenous cortisol production
- Pituitary tumor (85% of cases) producing excessive adrenocorticotrophic hormone (ACTH)
- Adrenal tumor (15% of cases) producing excessive cortisol
- Iatrogenic administration of exogenous glucocorticoids (iatrogenic hyperadrenocorticism).
Clinical signs
Hyperadrenocorticism is a slowly progressive disease with signs that vary in severity depending on the duration and degree of cortisol excess. Clinical signs are similar to diabetes mellitus:
- Polyuria
- Polydipsia
- Polyphagia
In addition, dogs frequently have a pot-bellied appearance and alopecia or other skin and/or coat changes. Diabetes mellitus may develop secondary to hyperadrenocorticism, as a result of the insulin resistance caused by cortisol excess.
Treatment
Hyperadrenocorticism can be treated medically or surgically. Concurrent diabetes mellitus requires insulin treatment.Pancreatitis
Pancreatitis is inflammation of the pancreas. Digestive enzymes leak into and damage the surrounding pancreatic tissues.
Aetiology
In most cases, the cause of pancreatitis is idiopathic. Other predisposing factors may be:
- High-fat, low-protein diet
- Other diseases (Cushing's syndrome, diabetes mellitus)
Risk factors for pancreatitis include:- Breed—Miniature Schnauzer, Miniature Poodle, and Cocker Spaniel are at higher risk
- Obesity
- Cushing's disease
- Chronic renal failure
Acute pancreatitis may produce temporary diabetes mellitus and if there is extensive pancreatic necrosis, this may become permanent. A similar situation can arise if there is pancreatic neoplasia.

Caninsulin® 40 IU/ml Suspension for Injection contains porcine insulin.POM-V
Further information is available from the SPC, datasheet or package leaflet.
Advice should be sought from the medicine prescriber.
Prescription decisions are for the person issuing the prescription alone.
Use Medicines Responsibly.
MSD Animal Health UK Limited, Walton Manor, Walton, Milton Keynes, MK7 7AJ, UK
Registered in England & Wales no. 946942
References
- Miller E. Long-term monitoring of the diabetic dog and cat: clinical signs, serial blood glucose determinations, urine glucose and glycated blood proteins. Vet Clin North Am Small Anim Pract 1995;25(3):571-84.
- Adapted from Rijnberk A. Clinical Endocrinology of Dogs and Cats. Kluwer Academic Publishers, NL. 1996:222.
- Lust E, van Esch K, Slingerland LI, Kooistra HS, Horspool LJI. Survey of Veterinary Professional and Pet Owner VetPen User Experience. Presented at the 42nd WSAVA and FECAVA 23rd Eurocongress; Copenhagen, Denmark; 25-28 September 2017
- Burgaud, S., Riant, S. & Piau, N. (2012). Comparative laboratory evolution of dose delivery using a veterinary insulin pen. WSAVA Poster
- American Diabetes Association (Position Statement). Hyperglycemic crises in patients with diabetes mellitus. Diabetes Care 2001;24(1):154–61.
- Amie Koenig. Endocrine Emergencies in Dogs and Cats. Vet Clin Small Anim 43 (2013) 869–897
- Amie Koenig. Endocrine Emergencies in Dogs and Cats. Vet Clin Small Anim 43 (2013) 869–897



